
Solitary Confinement in U.S. Immigration Prisons, 2013-2017
By Konrad Franco (UC Davis), Caitlin Patler (UC Davis), and Keramet Reiter (UC Irvine)
The Facts:
U.S. Immigration and Customs Enforcement (ICE) imprisoned a high record of up to 52,000 people per day in 2019, yet information on conditions of confinement is extremely limited. One of the least understood practices is solitary confinement, leading scholars to describe the practice as a black box within a black box.1 Being placed in solitary confinement often means an immigrant is locked in a windowless cell, alone for 22-23 hours each day, sometimes for weeks or months at a time, and often with long-term negative effects.2, 3 Indeed, the United Nations argues that solitary confinement in excess of 15 days should be banned, and should never be permitted for individuals with mental illness, because it can amount to cruel, inhuman, or degrading treatment, or even torture, in violation of international human rights standards.4
In a new paper, recently published in Punishment & Society, we provide the first systematic, national analysis of administrative records of solitary confinement in immigration detention.5 We examine patterns in who experiences solitary confinement, ICE’s stated reason for confinement, and the duration of confinement. Although ICE has published guidelines for the use of solitary confinement in its facilities, we find several inconsistencies (and potential human rights violations) in the application of this punitive practice:
-
Immigrants from countries in Africa or the Caribbean make up a vastly disproportionate share of solitary confinement cases, relative to their share of the detained population overall.
-
Immigrants with mental illness are also overrepresented in solitary confinement. Moreover, cases involving people with a mental illness are more likely to occur without any infraction (i.e., for non-disciplinary reasons) and are predicted to last longer, compared to cases that involve people without a mental illness.
-
Solitary confinement is applied inconsistently across regions and types of facilities. In particular, privately operated facilities are more likely to place an individual in solitary confinement without an infraction—and for longer—than publicly operated facilities. This suggests broad discretion over who goes to solitary, why, and for how long, in spite of federal guidelines
The Data:
We merged three administrative datasets from ICE, gathered via Freedom of Information Act (FOIA) requests: (a) all cases of solitary confinement from September 2013 to March 2017 lasting 14 days or longer (N=5,327), (b) individual-level data on every person detained by ICE during fiscal year 2015 (N=355,678), and (c) facility-level data on all ICE detention facilities from 2009 to 2018 (N=102 facilities). We group ICE’s stated placement reasons into two categories: solitary confinement without an infraction (i.e., “disciplinary”) and “solitary confinement with an infraction (i.e., “administrative”). We measure confinement length in days. Our analyses control for demographic and facility-level characteristics of solitary confinement cases.
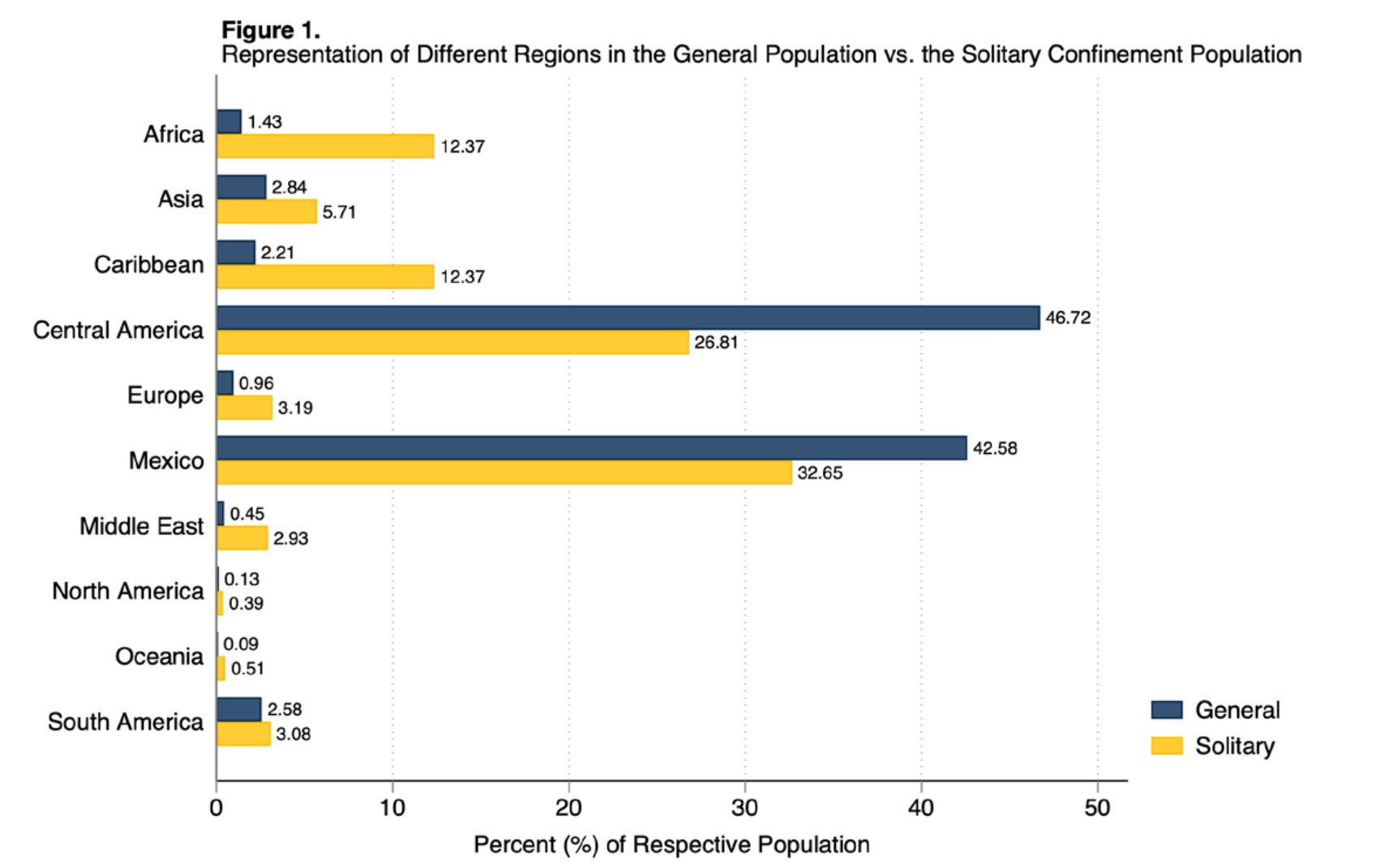
Figure 1 shows the composition of the general ICE detention population versus the solitary confinement population by country of origin region. African and Caribbean immigrants are overrepresented by a factor of 6.8 in solitary confinement cases when compared to the population of all detained people (24.74 vs. 3.64%, respectively).

Figure 2 shows the predicted probability of solitary confinement occurring without a disciplinary infraction. Cases involving people with a mental illness are more likely to occur without any infraction, compared to cases that involve people without a mental illness (predicted probability of 63% vs. 43%, respectively). Privately operated facilities are also more likely to use solitary confinement without an infraction, compared to publicly run detention facilities like local jails (predicted probability of 53% vs. 35%, respectively).
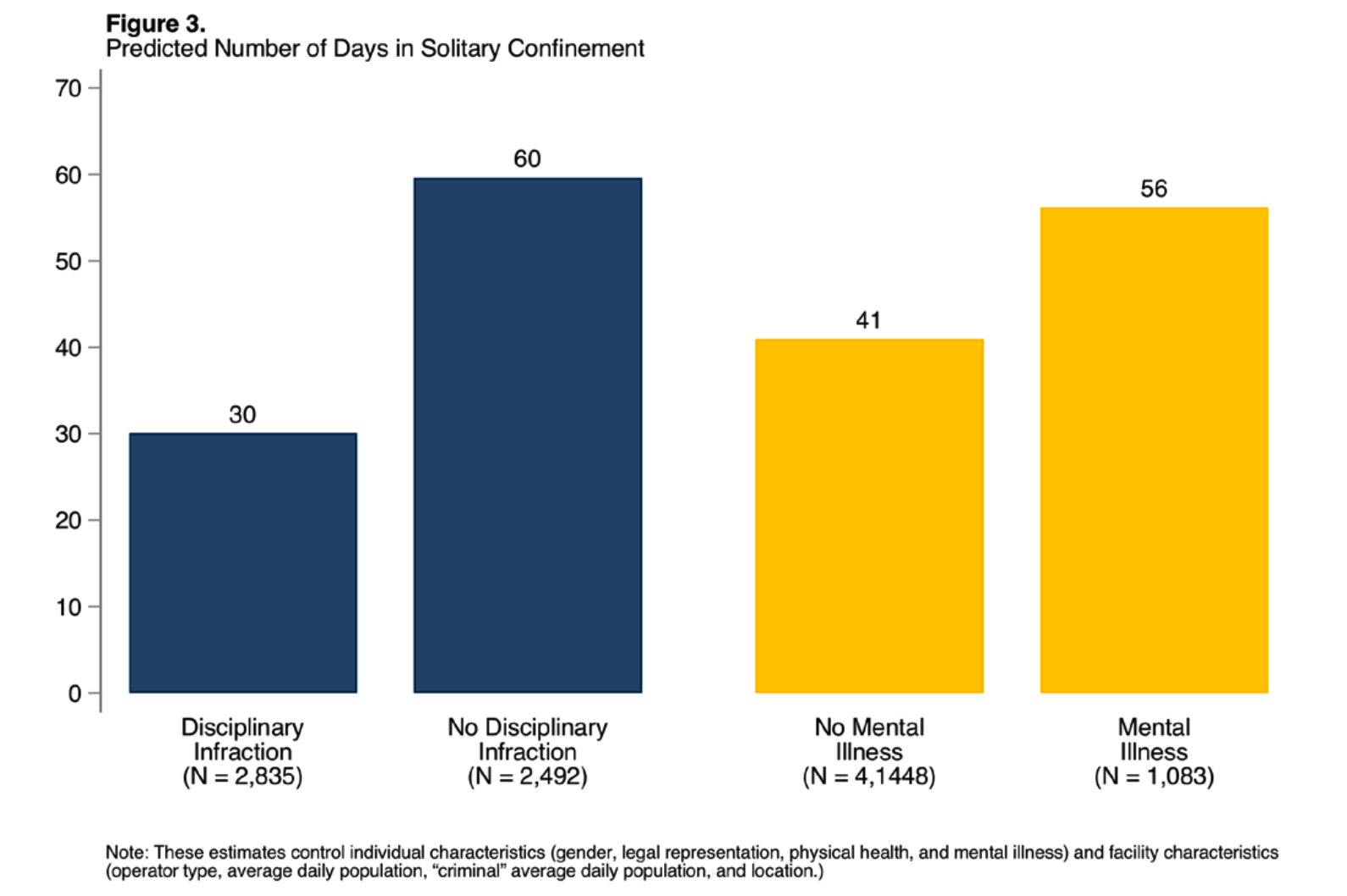
Figure 3 shows the predicted length (in days) of solitary confinement. Cases involving individuals with a mental illness are predicted to last more than two weeks longer, on average, than cases involving individuals without mental illness (56 vs. 41 days, respectively). Cases that are initiated without a disciplinary infraction last a month longer, on average than cases with an infraction (60 vs. 30 days, respectively).
Conclusion
Documenting and analyzing solitary confinement use in immigration detention is timely and salient, especially given the serious human rights violations associated with the
practice. While a major national and international movement is curbing both the frequency and duration of solitary confinement placements in prisons,6 our data suggest that no such curbs exist on solitary confinement use in immigration detention. Although ICE’s guidelines for solitary confinement mandate “careful consideration of alternatives” to solitary confinement placement, especially for individuals with “special vulnerabilit[ies],”7 we find that vulnerable (e.g. mentally ill) and historically marginalized populations (e.g. immigrants from majority-Black countries) are at greater risk of experiencing this punitive practice.
What should this mean for policy?
• The federal government should follow guidelines8
from the United Nations regarding solitary confinement, dramatically limiting lengths-of-
stay, if not abolishing the practice
altogether, especially for the most vulnerable detainees, such as those with mental illnesses.
• As long as the practice continues, the government must establish increased oversight:
– Data on the frequency and characteristics of solitary confinement should be made regularly and publicly available in order to more easily track patterns and mitigate harm.
– ICE should establish more robust procedural protections to ensure that detainees know why they are being placed in solitary confinement, have regular reviews of their placement, and have opportunities and resources to challenge these placements.
• Government oversight agencies should interrogate the disproportionate use of solitary confinement among immigrants from Africa and the Caribbean.
• In the absence of federal policy to ensure oversight, states should mandate that facilities within their borders comply with federal guidelines and adhere to the basic detention standards outlined in their sub-contracts. States can use their powers to require oversight of facilities within their borders. California’s AB 3228, signed into law in October 2020, is an example of such legislation.
View and Download this Immigration Fact
- 1Patler, C., Sacha, J.O. & Branic, N. (2018). The black box within a black box: Solitary confinement practices in a subset of U.S. immigrant detention facilities. Journal of Popula- tion Research, 35: 435–465.
- 2Schwellenback N, Steinle M, Hawkins K, et al. (2019) Isolated: ICE Confines Some Detainees with Mental Illness in Solitary for Months. Project on Government Oversight, 14 August.
- 3Woodman S, Saleh M, Rappleye H, et al. (2019) Solitary Voices: Thousands of Immigrants Suffer in Solitary Confinement in ICE Detention. The Intercept, 20 May.
- 4United Nations Standard Minimum Rules for the Treatment of Prisoners (2016) A/RES/70/175.
- 5Franco, K., Patler, C., & Reiter, K. (In Press). Punishing Status and the Punishment Status Quo: Solitary Confinement in U.S. Immigration Detention Facilities, 2013-2017. Punishment & Society. https://doi.org/10.1177/1462474520967804
- 6Reiter, K.; Blair, T. (2018). Superlative subjects, institutional futility, and the limits of punishment. Berkeley Journal of Criminal Law, 23(3): 162-193.
- 7U.S. Immigration and Customs Enforcement (ICE). (2013). “Review of the Use of Segregation for ICE Detainees.” Memo 11065.1.
- 8United Nations Standard Minimum Rules for the Treatment of Prisoners (2016) A/RES/70/175.